Clinical documentation is the backbone of safe, continuous healthcare. In India’s busy OPDs and overstretched hospitals, documentation often becomes the victim of time pressure.
This article explores how AI-driven documentation tools — from speech-to-text scribes to automated SOAP-note generators — will reshape clinical workflows in India by 2030,
the obstacles to overcome, and what stakeholders should do next.

On this page
- Where India stands today
- Key AI technologies shaping documentation
- Why AI scribes fit India well
- Opportunities and benefits
- Challenges and risks
- Roadmap 2025–2030
- Use cases and recommendations
- FAQ
Introduction — why documentation matters now
Clinical documentation underpins patient safety, continuity of care and health-system planning. When clinicians are forced to choose between time with a patient and time spent documenting, the record often become incomplete or delayed. That missing data affects clinical decisions, referrals, billing, and public health reporting — and it contributes to clinician burnout. AI promises to change that balance by automating routine tasks and letting clinicians focus on care.
Where India stands today
India already has two critical strengths that make AI-led documentation realistic:
- National digital health infrastructure. The Ayushman Bharat Digital Mission (ABDM) is creating a digital backbone and health identifiers that can enable interoperability and consented data flows — essential for many AI workflows.
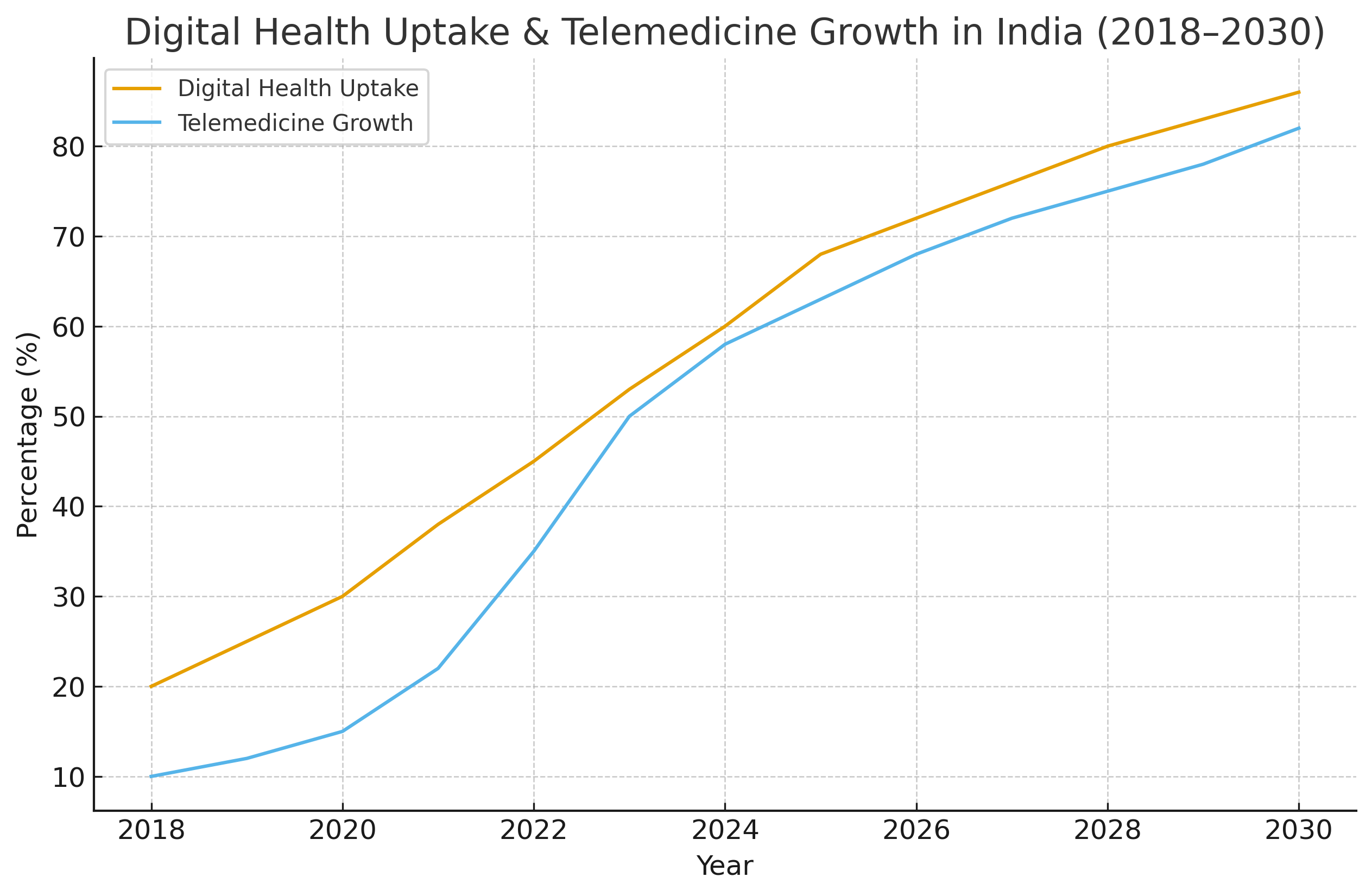
- Fast-growing telemedicine and EMR adoption. As teleconsultations and electronic records increase, so does the availability of structured data and audio sources AI systems can use to learn and operate.
Key AI technologies that will shape documentation by 2030
Several technical building blocks will move from pilots to everyday use in clinics:
- Advanced speech-to-text tuned for Indian English, regional accents, and medical vocabulary to reduce correction time.
- Clinical natural language understanding (NLU) that extracts problems, medications, allergies and timelines and maps them to structured terminologies (ICD/SNOMED).
- Automated SOAP and structured-note generation producing editable clinician-ready notes instantly.
- Context-aware summarization to create succinct longitudinal summaries for handoffs and referrals.
- EMR connectors and API-first integrations to write notes directly into electronic medical records and populate billing codes.
- Clinical decision-support overlays — explainable, lightweight alerts embedded into generated notes for safety.
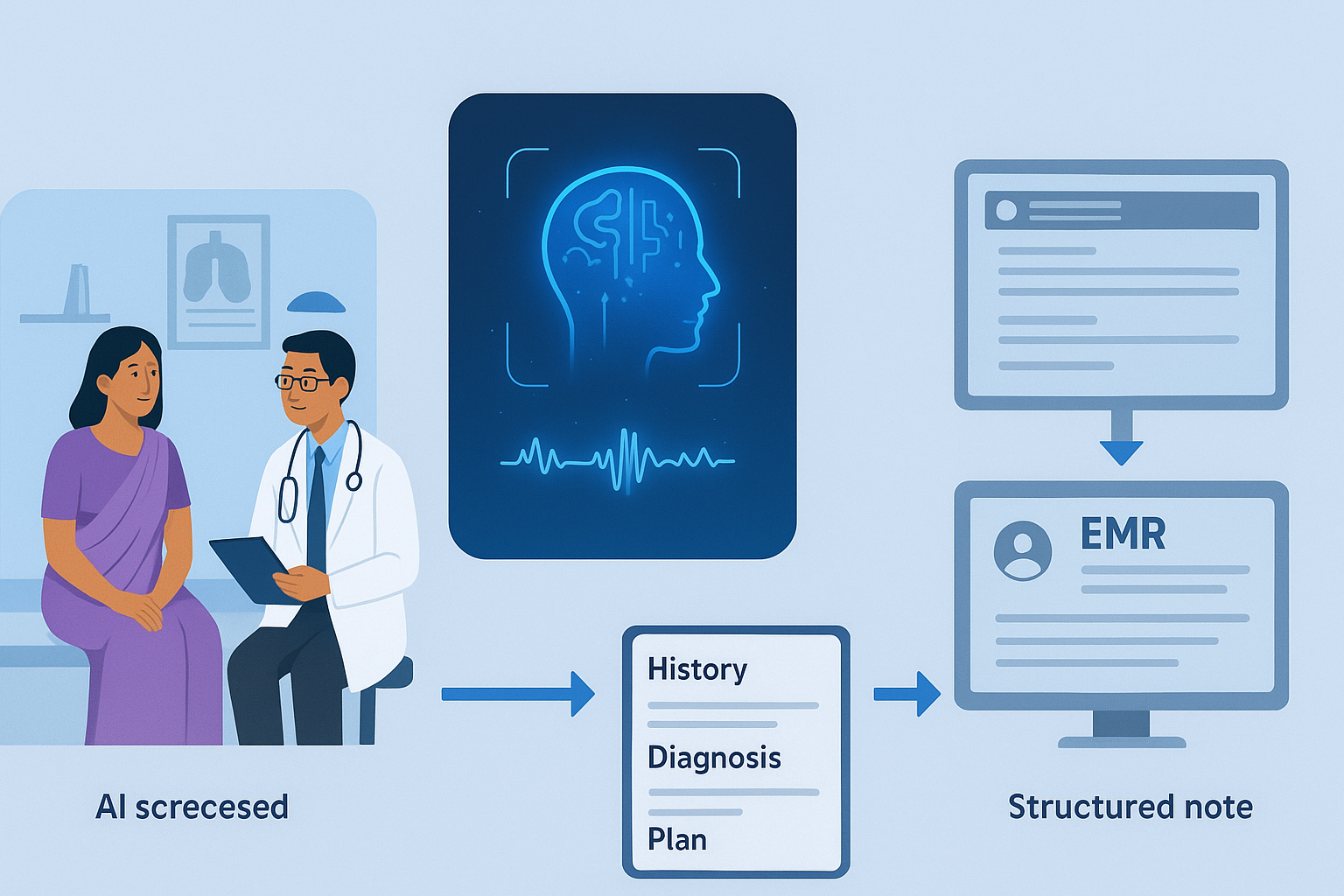
How an AI scribe integrates into a clinical workflow.
Why AI scribes are especially suitable for India
- High patient volumes. Even small per-consultation time savings scale to large productivity gains in busy clinics and hospitals.
- Rapid telemedicine uptake. Teleconsultations naturally provide audio data for AI to transcribe and summarize.
- Government push for interoperability. ABHA/ABDM identifiers and APIs, where available, allow AI systems to access consented longitudinal records to improve note quality.
Important opportunities (what AI can deliver by 2030)
- Clinician time savings. AI scribes can shift documentation burden away from clinicians, freeing time for patient care.
- Improved data quality. Structured notes enable better research, outcome tracking, and public-health analytics.
- Better patient experience. Less waiting, clearer follow-up instructions, and portable histories across providers.
- Cost efficiencies. Reduced manual transcription, fewer errors, and faster billing processes.
- Rural reach. AI can enable non-physician providers to create standardized documentation and extend specialist guidance.
Real challenges and risks to solve
- Data privacy and consent. Recording and processing patient conversations requires clear consent capture and secure storage aligned with Indian regulations and local norms.
- Language and dialect diversity. India’s many languages and code-switching require models trained on diverse corpora.
- Clinical accuracy and liability. AI notes must be auditable and editable; the clinician must retain responsibility for final content and be able to correct errors.
- Interoperability gaps. Many smaller clinics still operate on paper or isolated software; bridging heterogeneity is a major implementation task.
- Trust and workflow fit. Poorly integrated tools that create extra correction work will be rejected by clinicians.
- Cost & business models. Affordable pricing strategies are necessary for adoption by small clinics and rural providers.
A plausible 2025–2030 roadmap for India
2024–2026 — pilots and integration
Wider pilots in tertiary centres and private hospital chains focused on local languages, EMR integrations, and telemedicine attachments. Regulatory sandboxes and validation studies grow.
2026–2028 — scaling and specialization
AI scribes become common in urban hospitals and regional networks. Specialized modules (pediatrics, OB/GYN, orthopedics) are introduced and systems route structured outputs to registries and quality programs.
2028–2030 — normalization and ecosystem effects
Seamless EMR integrations, ABHA-linked histories and routine use in primary care. At this stage insurers and public programs may start accepting AI-generated notes for claims and reporting, producing measurable productivity and quality improvements.
Use cases that will reach maturity first
- OPD scribing in private hospitals and urban clinics — high ROI due to volume and willingness to pay.
- Teleconsultation transcription and summaries — audio exists already, making this a natural first win.
- Referral and discharge summaries — repetitive and structured tasks are ideal for automation.
- Primary-care support for community health workers — AI helps generate standardized records for referrals.

Priority use cases for AI documentation.
Recommendations for stakeholders
For clinicians
Start with co-designed pilots. Choose tools that allow editing, version history and easy export to your EMR. Prioritise vendors with local language competence and clinician co-design processes.
For hospital administrators
Integrate AI scribes as workflow changes — not as add-ons. Budget for training, change management and clear EMR integration plans. Prefer API-first vendors and insist on audit trails.
For policymakers & regulators
Define clear rules for consent, data residency and auditable trails for AI records. Offer regulatory sandboxes for safe innovation and rapid validation.
For startups and vendors
Focus on explainability, clinician control, low bandwidth performance and tiered pricing for smaller clinics. Prioritise interoperability with ABDM/ABHA and major EMRs.
FAQ
- Will AI replace human medical scribes in India by 2030?
- Unlikely to fully replace human scribes everywhere. AI will automate routine documentation, but human oversight, clinical judgement, and complex case handling will remain essential.
- Is patient conversation data safe with AI scribes?
- Safety depends on vendor practices and legal frameworks. Use vendors with end-to-end encryption, clear consent capture, and data residency options.
- How will AI handle India’s many languages?
- Multilingual and code-switching models are emerging, but wide coverage requires dedicated training data and continuous testing.
Final Words — a realistic, hopeful view
By 2030, AI will be an integrated component of India’s clinical infrastructure. With ABHA/ABDM, telemedicine growth, and improving models, this is a unique window to transform documentation from a burden into an asset. Success requires addressing language diversity, privacy, clinician trust, and interoperability. For those who approach the task with pragmatic pilots, strong clinical partnerships and transparent governance, the payoff will be cleaner data, happier clinicians and smoother patient journeys.